
Note: Some examples in this article are drawn from real therapeutic themes, with all personal identifiers removed to protect privacy.
In therapy, we often meet clients who do not describe themselves as anxious at first. They say they are careful, thoughtful, responsible, or simply trying to stay ahead of what might go wrong. But as the conversation unfolds, a familiar pattern appears: the mind has started treating possibility like certainty. A text goes unanswered and suddenly there are fake scenarios in your head about rejection, conflict, or loss. A small mistake at work becomes a full internal movie about being fired from a new job, disappointing loved ones, or confirming old fears about worthiness. That is the terrain of worst-case scenario thinking, and in overthinking psychology, it often sits at the intersection of fear, habit, and an exhausted nervous system.
From a clinical perspective, this pattern is common among people dealing with Social burnout, chronic stress, and other forms of emotional overload. When someone has been carrying the emotional burden of being the strong one, the mind can slip into constant scanning for danger, disappointment, or relational rupture. That scanning may look like People pleasing, Conflict avoidance, Over apologizing, Validation seeking, or difficult conversation avoidance on the outside, while internally it feels like a relentless rehearsal for the worst possible outcome. In everyday practice, we also see it linked to boundary setting struggles, criticism sensitivity, and the deeper fear that if something goes wrong, there will be no room to recover.
Here’s what Zainib says about a firsthand experience with a client that has this mindset:
One of my clients described this as how it feels like he's already in the worst part of an experience or outcome sort of situation without even starting it or beginning or moving towards it. It feels so real that fear he's experiencing is so embodied, so factual, quite unquote, that he's already experienced the situation and that he just doesn't go towards it. Considering that this was a 32-year-old male who's a high-functioning professional , it gave him a lot of discomfort to have these experiences with specific situations and also very confusing for him because he was confident in so many ways in other places in his life.
At its core, worst-case scenario thinking is a form of catastrophizing, which clinicians describe as a cognitive distortion in which the mind jumps quickly to the most threatening interpretation of a situation. It is not the same as healthy planning or realistic risk assessment. Healthy planning says, “Something could go wrong, so I will prepare.” Catastrophic thinking says, “Something will go wrong, and it will probably end badly.” That shift matters because it turns uncertainty into danger and possibility into emotional certainty. Cleveland Clinic describes catastrophizing in similar terms, as a pattern of leaping to extreme conclusions and assuming the most harmful ending, even when evidence is limited.
This pattern is not itself a diagnosis. It is better understood as a process that can appear across multiple presentations, including anxiety disorders, ocd, obsessive-compulsive disorder, depression, trauma responses, and chronic stress. The National Institute of Mental Health describes OCD as involving intrusive, unwanted, recurring thoughts and repetitive behaviors or mental acts, while NIMH’s anxiety materials describe excessive worry that is difficult to control and disruptive to functioning. In other words, catastrophic thoughts are often a feature of a broader mental health condition, not proof of one specific disorder on their own.
In therapy, the distinction we usually make is between realistic caution and distorted escalation. A person can think, “I should prepare for a hard conversation,” without imagining abandonment, humiliation, or disaster. But when the mind has learned to anticipate negative outcomes, every ambiguous moment begins to feel like a threat. That is where negative thinking, rumination, and body-based activation start to reinforce one another. The longer the cycle runs, the more it can look like personality, when in reality it is often a treatable pattern shaped by stress, history, and repetition.
Here’s what Zainib generally thoughts on the issue:
One of the ways I like to help clients understand this issue is label it as a way of thinking that's unhelpful, unprotective, called catastrophization. But what's really important is I highlight that even as uncomfortable as it is, it's just highlighting how protective people are of themselves. This is the first step to understanding how to combat the issue as worst case scenario thinking stems from trying to protect oneself from.

One reason this pattern is so sticky is that it can feel rational from the inside. Clients often do not say, “I am catastrophizing.” They say, “I’m just being realistic,” or “I need to think this through.” But over time, there are recognizable signs. The first is automatic escalation: a setback becomes proof of collapse, a pause becomes proof of rejection, and a similar situation from the past becomes evidence that the same pain is about to repeat.
Another sign is persistent what if spiraling, even when no action is being taken. A client may replay a meeting, a dating exchange, a family interaction, or a comment from a manager until it expands into a chain of imagined disasters. This often creates decision fatigue, because the person is not only choosing what to do but also trying to prevent every imagined mistake before it happens. They may check for reassurance, avoid replying, draft and redraft messages, or withdraw socially after emotional flooding has made it hard to think clearly. In clients already struggling with social burnout, this turns ordinary interaction into a high-cost activity.
We also watch for body-based signs. The NHS describes anxiety and PTSD-related arousal as involving restlessness, trouble relaxing, poor sleep, irritability, tension, and feeling “on edge.” When a person is living with hypervigilance, the body often reacts before the thinking mind can slow anything down. That is why worst-case thinking is not only cognitive; it is also physiological. Tight chest, shallow breathing, stomach discomfort, muscle tension, and racing thoughts can all become part of the same loop, affecting both physical symptoms and broader physical health over time.
One key clinical marker is impact. Occasional fear is part of being human. But when this pattern consistently disrupts daily life, relationships, work, sleep, concentration, or the ability to enjoy the present moment, it is no longer just a bad habit. It is a signal that emotional resources are overtaxed and that support may be needed.
Here’s a legitimate example from Zainib about the signs:
Another one of my clients, a 40-year-old new mother, once reported to me that she was assessing and reflecting on her experience of worst-case scenario thinking, which she had been experiencing for almost nine months during the phase of her baby waking frequently. At the time, her baby was about four months old. Now, there is an adjustment period, of course, to new motherhood, but what is very important for us is understanding the frequency and the intensity of the experience, because that helps us assess the type of support that is needed. In her case, this included psychiatric support as well as additional psychotherapy, because she had been experiencing such high-intensity anxiety, often tied to fears of difficult things happening to her baby. Even though she explored medication and took it for about a year, even if medication is not considered, it is helpful to have the support of a multidisciplinary team to make sure that we are looking at the person as a whole. This ensures that the treatment and the experience they are concerned about are supported and addressed appropriately.
The short answer is that the brain usually develops this pattern for a reason. For many people, it begins as an attempt to stay prepared. If life has taught you that bad things can happen unexpectedly, then scanning ahead may feel safer than relaxing. In that sense, rumination causes and catastrophizing are often less about irrationality than about an overworked safety system. The problem is that a strategy meant to protect emotional well-being can end up damaging it.
Anxiety is one major driver. NIMH notes that generalized anxiety involves excessive worry that is difficult to control, along with restlessness, irritability, trouble sleeping, and trouble concentrating. When anxiety is chronic, the mind starts scanning constantly for threat, and uncertainty becomes hard to tolerate. A delayed reply, an unclear tone, or a schedule change can quickly trigger the expectation of the worst fears coming true. That is why worst-case scenario thinking is often less about logic than about the nervous system trying to get certainty at any cost.
Past learning matters too. People with trauma histories may have nervous systems trained to anticipate danger, even when danger is not currently present. The NHS notes that post-traumatic stress disorder can involve feeling on edge, easily startled, and constantly aware of threats, while PTSD materials from VA sources describe lingering hypervigilance even after progress in treatment. When that history is present, catastrophic thinking may feel like vigilance rather than fear. The mind is not simply “thinking negatively”; it may be reenacting an old survival strategy shaped by past experiences.
Cognitive style also plays a role. Once a person begins to interpret uncertainty through a lens of danger, negative thoughts start linking together quickly. One fear recruits another. One possible mistake becomes proof of many future failures. That chain reaction is what many clients mean when they say they can feel one bad thought turning into something much bigger before they can stop it. It is also why treatment often focuses not on arguing with every thought, but on slowing the process enough to notice it and reframe it.
Finally, this pattern often becomes relational. Someone who has learned to survive through people pleasing, conflict avoidance, or emotional self-erasure may catastrophize around disapproval, criticism, or emotional distance. They may become preoccupied with whether they sounded rude, whether they upset someone, or whether a partner who feels emotionally unavailable is about to pull away. In practice, we often see this tied to self-esteem, attachment insecurity, and the hidden exhaustion of trying to be easy, agreeable, and un-needy while feeling overwhelmed inside.
Here are Zainib’s thoughts on the core elements of worst case scenario thinking:
We need to start to have a conversation around the protective aspects of such a distressing experience. When we understand the protective response, as well as the reasons behind why a part of us has felt like it needed to show up in this way and prepare us, it also helps us understand the history of when this experience was needed and that helps us develop self-compassion for ourselves. I see this over and over again within maybe three or four sessions, people experience such a lesson intensively by just simply understanding and turning towards that part and understanding their history so they're not fragmented and confused. And of course, there is the guided therapy needed for us to turn towards that part because there are parts of us that also don't like the over-thinking (which overlaps with worst case scenario thinking).
Worst-case thinking can look mental at first, but its effects are broad. When the mind is repeatedly rehearsing disaster, the body often follows. Sleep gets lighter, concentration narrows, social interactions feel more effortful, and ordinary decisions begin to cost more energy. Over time, that reduces quality of life, drains well-being, and can pull someone away from the relationships and activities that support recovery.
This is especially important when we think about social burnout. A client who is already depleted may start approaching every invitation, message, or conversation as another test to fail. They may cancel plans, avoid difficult conversations, and default to silence because emotional recovery takes too long afterward. What looks like withdrawal can actually be a combination of catastrophic anticipation, self-sabotaging protection, and limited emotional bandwidth. In that state, even supportive relationships can start to feel demanding, and loved ones may misread exhaustion as disinterest.
Relationships often take a hit because catastrophic thinking changes how people interpret ambiguity. A neutral tone becomes rejection. A disagreement becomes rupture. A need for space becomes proof that someone is leaving. That can intensify over apologizing, reassurance-seeking, or emotional shutdown, especially in clients who already carry criticism sensitivity or fear becoming a burden. In session, we sometimes see the irony that the very strategies meant to prevent disconnection end up creating more strain.
The internal cost is just as significant. Constant threat prediction erodes trust in one’s own judgment, making it harder to choose, rest, or feel settled. Many clients describe a shrinking world: fewer risks, less spontaneity, more checking, more avoidance, and less room for joy. That is why treatment is not only about reducing fear. It is also about restoring self-compassion, emotional regulation, and enough safety that a person can re-enter life rather than simply brace against it.
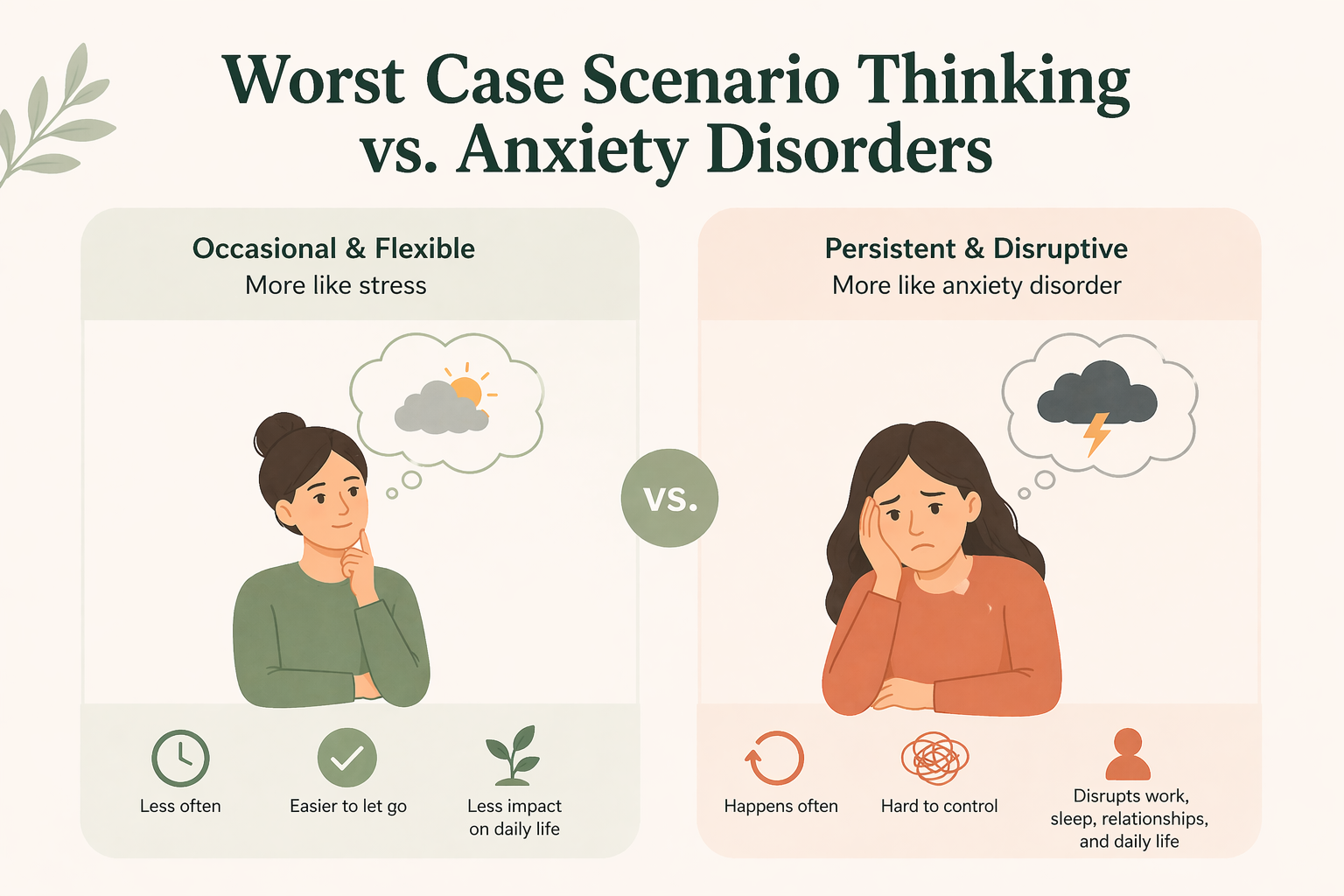
The clinical question is not whether the thought appears, but how often it appears, how convincing it feels, and how much it shapes behaviour. When worst-case thinking is occasional and flexible, it may reflect stress more than disorder. When it becomes persistent, distressing, difficult to control, and disruptive to work, sleep, relationships, or functioning, it starts to overlap more clearly with anxiety disorders and related concerns.
For example, generalized anxiety is marked by excessive worry across multiple domains of life, while OCD involves intrusive, unwanted thoughts and often repetitive acts or mental rituals aimed at reducing distress. Some people with obsessive-compulsive disorder get caught in “what if” spirals that assume danger, contamination, harm, or moral failure, then seek reassurance or perform rituals to feel temporarily safer. In that context, worst-case thinking is not just a style of thinking; it can become part of an obsession-compulsion loop. NIMH and the NHS both describe OCD as involving recurrent intrusive thoughts and repetitive responses that temporarily relieve distress, which is one reason catastrophic thinking can feel so sticky in OCD presentations. and
Trauma is another overlap worth naming carefully. Not everyone with catastrophic thinking has trauma, and not everyone with trauma catastrophizes in the same way. But in post-traumatic stress disorder, a mind shaped by danger may continue scanning for future harm long after the original event is over. When that happens, treatment has to respect that the pattern may have been adaptive once, even if it is now limiting emotional well-being.
The most effective work usually begins by dropping the idea that you must win an argument with every fear. In therapy, we are often less interested in proving a thought wrong than in weakening the process that makes it so believable. That is where cognitive behavioural therapy and other structured approaches become useful. Cleveland Clinic identifies CBT as a standard treatment for catastrophizing, and the NHS describes CBT self-help techniques as ways of working with worries and unhelpful thoughts rather than simply trying to suppress them.
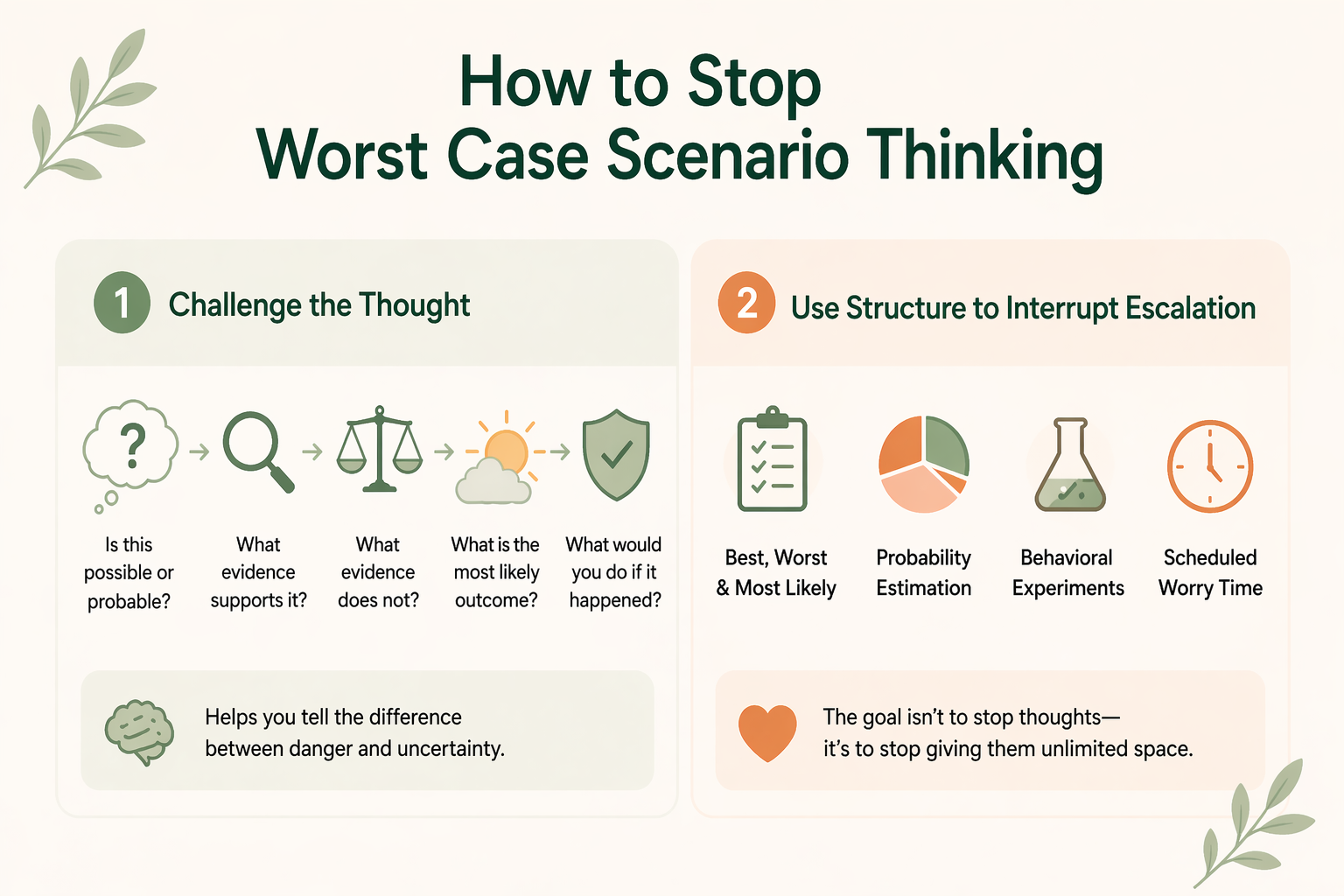
One core cbt move is cognitive restructuring. A therapist might ask: Is this thought possible, or is it probable? What evidence supports it? What evidence does not? If the mind has locked onto the worst possible outcome, what is the most likely outcome, and what would you do if the feared outcome actually happened? This does not erase fear, but it teaches the brain to distinguish danger from uncertainty. It also helps clients reframe the difference between being prepared and being trapped in prediction.
Another useful approach is to interrupt escalation with structure. Many therapists use some version of the “best, worst, and most likely” exercise because it forces the mind out of all-or-nothing thinking. Others use probability estimation, behavioral experiments, or scheduled worry time. The NHS’s “tackling your worries” materials include structured worry techniques for managing repetitive worry, and in session these can help clients see that the problem is not that they have thoughts, but that the thoughts are taking up unlimited space.
Grounding matters because the body usually enters the cycle before insight arrives. If the nervous system is already activated, insight alone may not feel accessible. That is why therapists often pair cognitive work with breathing, sensory grounding, movement, or mindfulness that brings attention back to the present moment. The NHS notes that mindfulness can help with stress, anxiety, and depression for many people, though it is not right for everyone, which is an important tradeoff to acknowledge.
For clients with social burnout, relational patterns also need attention. Catastrophic thinking often quiets down when people become less entangled in pleasing people, more honest about limits, and more willing to tolerate small amounts of relational discomfort without assuming catastrophe. That may mean reducing over apologizing, practicing direct communication, challenging difficult conversation avoidance, and building more sustainable self-care rather than performing emotional stability for everyone else. When those changes are made carefully, they do not just reduce symptoms; they increase freedom.
Here’s a final example from Zainib:
My recent session with one of my clients, who is a recent graduate in her late 20s, and has just entered the workforce and has been experiencing a lot of workplace anxiety. After our work, understanding why that part of her shows up, and the history of that part of her that's connected to some difficult experiences that she had in her childhood, she's been able to have a bit of a conversation with that part to help turn herself. With this self talk, she can use her prefrontal cortex or the parts of her brain that are not so activated by the emotion that is connected to the history of that experience. She can then offer herself the understanding of some of the facts in that situation that protective part of herself is not engaging with to help her better manage a situation, as she's feeling such a loss of anxiety. Of course, our work continues to be unburdening that part of her, healing some of those early childhood experiences, which has dramatically changed her anxiety, because at the end of the day, we're still going to get protective anxiety that might show up everyday, but the intensity and the frequency of it is what we're trying to diminish in her life.
Professional support is worth considering when worst-case thinking is persistent, distressing, or shaping major parts of life. If someone is avoiding social contact, repeatedly seeking reassurance, losing sleep, struggling at work, or feeling stuck in panic-like spirals, the issue is not just overthinking. It is a meaningful strain on functioning and a signal that more structured support may be useful. NHS and NIMH guidance both emphasize seeking help when anxiety is hard to cope with or begins interfering with life. This is especially true when catastrophic thinking is linked to compulsive checking, trauma symptoms, intrusive thoughts, severe avoidance, or deep drops in self-esteem and functioning. It can also matter when the person knows the fear is excessive but still cannot disengage from it. That gap between insight and relief is often where therapy becomes most helpful, because the work is not simply educational. It is experiential, relational, and skill-based.
At Wellnest, therapists can frame this work not as “stop being negative,” but as learning how to relate differently to fear, uncertainty, and internal threat cues. That shift reduces shame and makes room for change. It also fits the clinical reality that many clients already know their thought is extreme; what they need is help interrupting the loop that keeps it alive.
Get started by choosing a therapist at Wellnest!

Therapy helps because it offers more than reassurance. Reassurance may calm the system briefly, but it can also teach the brain to keep outsourcing certainty. Good therapy instead builds the capacity to stay with uncertainty without collapsing into catastrophe.
In CBT, the focus is often on noticing patterns, testing assumptions, and changing the behaviors that keep fear in place. In trauma-informed work, the focus may include helping the body recognize that the current moment is not the same as the past. In acceptance-based work, the goal may be to loosen the grip of thoughts without arguing with all of them. For clients whose catastrophic thinking shows up in avoidance, exposure-based methods can also help by gently testing feared situations in real life rather than treating every prediction as untouchable truth. NHS guidance for OCD treatment also highlights exposure and response prevention as a core therapy when obsessions and compulsions are part of the picture.
This work can be especially meaningful for clients who have spent years being “fine” for everyone else. When someone is carrying the emotional burden of being the strong one, therapy becomes one of the few places where they do not have to perform calm while internally preparing for collapse. That matters, because healing often begins when the person no longer has to fight fear alone or hide how much energy the fighting takes.
Catastrophizing is not caused by one single illness, and it is better understood as a thinking pattern than as a diagnosis by itself. It can appear across several conditions, including anxiety disorders, depression, trauma-related presentations, and obsessive-compulsive disorder, especially when intrusive thoughts and reassurance-seeking are part of the cycle. NIMH materials on generalized anxiety and OCD both describe recurring worry or intrusive thoughts that can make catastrophic interpretations feel hard to disengage from.
Usually because your brain is trying to protect you, even if it is doing so in a way that overshoots the mark. When the stress system is activated, the mind becomes more likely to scan for threat, imagine negative outcomes, and rehearse danger in advance. This is especially common when there has been chronic stress, hypervigilance, or difficult past experiences that taught the brain uncertainty might not be safe.
It is not a formal diagnostic trait of ADHD in the same way that inattention or impulsivity are. But CHADD notes that ADHD is often associated with emotional regulation difficulties, and some ADHD-focused clinical education materials discuss how cognitive distortions like catastrophizing can become more visible when stress, frustration, or co-occurring anxiety are high. So the careful answer is that catastrophizing is not an ADHD criterion, but it can show up more often in people with ADHD-related emotional dysregulation or co-occurring anxiety.
The goal is not to force the thought away but to change the process that keeps feeding it. CBT-based tools such as cognitive restructuring, probability checking, and “best, worst, most likely” thinking can help you separate possibility from probability. Many people also need grounding or mindfulness first, because if the body is already alarmed, it is much harder to reframe anything clearly.
It can be a symptom or feature of several clinical pictures, including anxiety, OCD, trauma responses, and periods of high stress or burnout. That is one reason clinicians look at the full pattern rather than the single thought. Frequency, intensity, compulsive responses, avoidance, and functional impact all help clarify whether catastrophizing is part of a broader mental health condition.
People catastrophize because the mind is trying to prepare for threat, control uncertainty, or avoid being blindsided. In the short term, this can feel like protection. In the long term, it often increases anxiety, drains emotional energy, and teaches the brain that uncertainty must always be treated like danger.
Because OCD thrives on doubt, threat, and the urgent need for certainty. NIMH and NHS descriptions of OCD both emphasize intrusive, recurring thoughts and repeated efforts to reduce distress, which can make “what if” thinking feel especially compelling. When a person with OCD imagines harm, contamination, or moral failure, the catastrophic interpretation often becomes the very thing that drives compulsions or reassurance-seeking.
It should, because one of the most important clinical truths is that catastrophic thinking is workable. It may feel automatic, but it is not fixed. With the right healthcare support, practice, and self-compassion, people can learn to recognize the pattern sooner, regulate the body more effectively, and build a more stable sense of internal safety.
Start by naming the fear clearly instead of letting it stay ambient and everywhere. Then ask whether the feared outcome is merely possible or actually likely, and what evidence you have for each. If your body is activated, return to the present moment first through grounding, breathing, movement, or another regulating strategy before trying to think your way out of the spiral.
They might be, but intrusive worst-case thoughts alone are not enough to tell. OCD becomes more likely when distressing thoughts are repetitive, unwanted, and followed by mental rituals, checking, reassurance-seeking, avoidance, or compulsive behaviors aimed at reducing anxiety. Because OCD can look different from person to person, it is best assessed in context rather than guessed from one symptom in isolation.
Yes, and that chain reaction is one of the defining features of catastrophizing. A single worry can quickly recruit older fears, unresolved memories, and assumptions about identity until the original situation barely resembles the conclusion. That is why treatment often focuses on process awareness: catching the jump from one thought to the next before the entire internal system is organized around danger.
Useful strategies include cognitive restructuring, scheduled worry time, reality testing, behavioral experiments, mindfulness, and reducing reassurance-seeking or avoidance. For clients with Social burnout, it can also help to address relational habits like Conflict avoidance, People pleasing, and Over apologizing, because those patterns often keep the fear cycle active. What works best usually depends on whether the person is dealing mostly with stress, OCD-like doubt, trauma activation, or generalized anxiety.
Common triggers include uncertainty, relational ambiguity, work pressure, health fears, major transitions, and reminders of past hurt. For some people the trigger is external, such as starting a new job or having a hard conversation. For others it is internal, such as fatigue, Emotional flooding, or feeling suddenly disconnected from loved ones.
It can intensify worry, increase avoidance, reduce confidence, worsen sleep, strain relationships, and erode quality of life. Over time, it may contribute to broader symptoms associated with anxiety, depression, burnout, and lower emotional well-being. It also consumes mental bandwidth, which is one reason so many clients describe feeling exhausted even when they have not “done” much outwardly.
Join our Nest to learn more about:

